While much of the current day anti-vaxx sentiment is rooted in conspiracy theories, some fears have real historical experiences underlying, which must be reckoned with. Aro Velmet looks into how a yellow fever vaccine, rolled out in French West Africa during World War II, may have killed thousands over more than four decades.
In 1944, the United Nations Relief and Rehabilitation Administration (UNRRA) mandated that all travellers arriving in regions where yellow fever was endemic should be inoculated against the disease. Two immunization options were on offer: a vaccine developed by the American Rockefeller Foundation, known as 17-D, or one with a ‘French strain’ of the virus developed in Dakar, the capital of the West African territories colonized by France.
That same year, in Brazzaville, French Equatorial Africa, seventeen children died after receiving the Dakar vaccine. They had contracted encephalitis. In 1951, twelve children inoculated with the same vaccine in Costa Rica also fell ill with encephalitis, and three fatalities were recorded. A year later, in British Nigeria, eighty-three cases were noted, leading to thirty-two fatalities.
Experts at the World Health Organization (WHO) investigated and debated these cases throughout the 1950s and 1960s. They concluded that the French strain of the vaccine was to blame, rather than contaminated batches or production errors. More cases followed: in 1965, 207 children were hospitalized with encephalitis and twenty-five died, again shortly after vaccination.
No surprises
French microbiologist Jean Laigret was invited to Nigeria to investigate these troubling events. In the 1930s, Laigret had been a leading researcher working on the Dakar vaccine. He had travelled through many colonial outposts of the Pasteur Institute – then, as now, France’s leading microbiological research laboratory.
But here was the troubling thing: Laigret was not surprised by what he saw in Nigeria. After visiting Lagos, he wrote: ‘I first observed meningoencephalitis following yellow fever vaccination in 1934. I have now seen more than ten such cases’.1 The Nigerian instances were no novelty. In fact, throughout the vaccine’s development process, researchers at the Pasteur Institute had repeatedly expressed concern over possible adverse effects the vaccine might have on some patients. These anxieties went unheeded. During World War II more than fifteen million people in French West Africa were vaccinated with the Dakar vaccine strain.
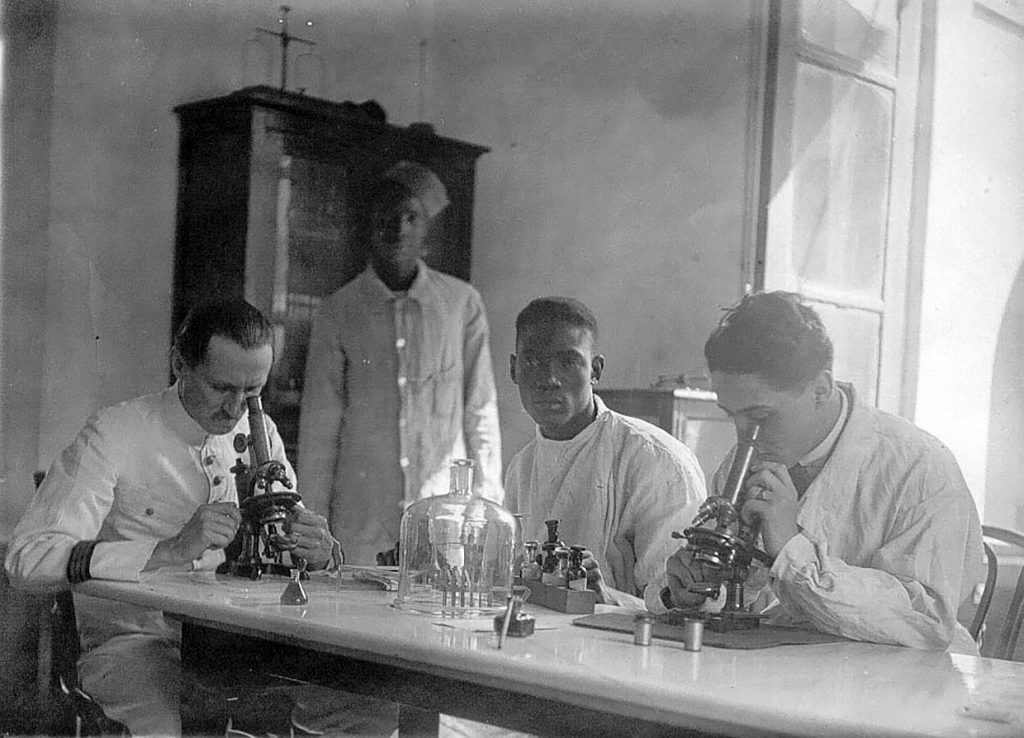
A bacteriological laboratory at a Dakar hospital, early 1930s.
The vaccine undoubtedly worked. Yellow fever had caused a serious epidemic in French West Africa in 1928, with smaller outbreaks in the years leading up to the war. But in the 1940s and 1950s, it was rarely diagnosed. As more and more countries chose to use the Rockefeller 17-D vaccine (the only one in use today), and as disasters surrounding the Dakar strain multiplied, inevitably questions were raised.
How was it that these adverse effects, observed by scientists in Paris and Dakar as early as 1934, had remained unaddressed for several decades, as tens of millions of vaccinations were performed?
The answer is linked to race and space.
During the vaccine’s development phase, Pastorian bacteriologists shifted their focus from the vaccination of vulnerable Europeans to a mass vaccination programme directed at Africans. In doing so, they had adopted a new set of development guidelines. These were less concerned with individual safety and, indeed, may have increased the likelihood of harmful outcomes.
While initial tests of the vaccine were conducted in Paris under the watchful eye of medics, critics and the international press, in West Africa trials were done on a mass scale. But here, lack of oversight and poor hospital infrastructure rendered adverse effects difficult to record. Many microbiologists working on the vaccine programme were concerned about potential damaging side effects but, in a colonial setting, harm caused to the health of black Africans was all but impossible to observe.
Arbitrary regulations
In surveying the development of the Dakar yellow fever vaccine, I have built on a body of scholarship concerned with ‘regulatory arbitrage’ – the practice of offshoring medical research from the globalized North to areas where looser regulations permit easier and cheaper clinical trials.
In recent decades, anything from diabetes and blood pressure medication to cocktails of drugs for HIV/AIDS developed in the US have been trialled in countries such as Poland, Ukraine or Brazil, where test subjects are easier to recruit and regulatory oversight is less stringent.
While differences between metropoles and peripheries are no longer as pronounced as in the colonial era, the practice – and harms – of regulatory arbitrage remain very real. Offshoring may profit from pharma-friendly legislation and lax oversight in receiving countries, but inequality of infrastructure also plays into the hands of drug developers.
Working in the colonies allowed microbiologists to make engineering choices that were not available to them in the metropole. Equally, the conditions of colonial infrastructure – the absence of hospitals, roads, clinics, and bureaucratic institutions – rendered adverse effects invisible.

Delegates of the 1928 yellow fever conference in Dakar, including Jean Laigret, Henry Beeuwkes, Watson Sellards, and Constant Mathis. Photo from the Rockefeller Archive Center.
The rocky road to a vaccine
Let us begin in Paris. In 1928, after a particularly deadly outbreak of yellow fever in West Africa, the world’s two preeminent medical research centres – the Rockefeller Foundation in New York and the Pasteur Institute in Paris – began developing vaccination programmes to stop this scourge of the tropics once and for all.
The race was on. By 1930, French researchers Jean Laigret and Georges Stefanopoulo, along with their American partner Andrew Watson Sellards, had made a significant breakthrough. They had developed an attenuated form of the yellow fever virus by cultivating it in the brains of lab mice, and selecting less virulent strains. After over 200 serial passages, they had evolved a virus that no longer caused symptomatic disease, which they believed would confer immunity against the virulent, ‘wild’ version of yellow fever.
The virus seemed to work well in animals – rhesus monkeys injected with the vaccine prototype no longer contracted yellow fever – and the researchers sought permission to proceed to human trials. Sellards even volunteered to be the first human test subject. But Émile Roux, head of the Pasteur Institute in Paris where the scientists worked, refused to give the go-ahead.
Laboratory accidents with yellow fever samples had led to the deaths of several researchers over the previous three years, and Roux did not consider the live virus vaccine to be safe enough for human testing. This could have marked the end of the French vaccination programme. But it did not.
Luckily for the researchers, Roux had a rival with a grudge. Charles Nicolle, the director of the Pasteur Institute in Tunis, had long been in an ongoing feud with the head of the Parisian parent institute. An ambitious colonial Pastorian, Nicolle criticized Roux for his aversion to profit, his reluctance to take risks and his inability to raise enough funds to restore the Pasteur Institute to its pre-World War I status and renown. He had made an unsuccessful bid to replace Roux as director of the Paris institute and, when this failed, sought to turn the Tunis institute into a competing hub of French bacteriology.
Hearing of Roux’s decision to halt trials of the yellow fever vaccine in Paris, Nicolle invited Laigret, Stefanopoulo and Sellards to Tunis. This was where, in 1931, the first clinical trials of the Pastorians’ vaccine began.
The trials gave little cause for optimism. While the first five Tunisian volunteers appeared to acquire immunity and showed no adverse reactions to the vaccine, the second set fared worse. Three out of the seven patients developed serious illnesses: high fever, neurological symptoms, and bloody sputum. Laigret became concerned.
Over the next few years, Laigret continued to work on improving the safety of the vaccine and reducing its virulence. He tested a number of different methods. He reduced the quantity of virus in an injection, exposed the virus-vaccine to low temperature, dried the preparation, coated the vaccine in egg yolk which increased its absorption time, and added two booster shots which enabled him to further reduce the concentration of the virus in a single shot.
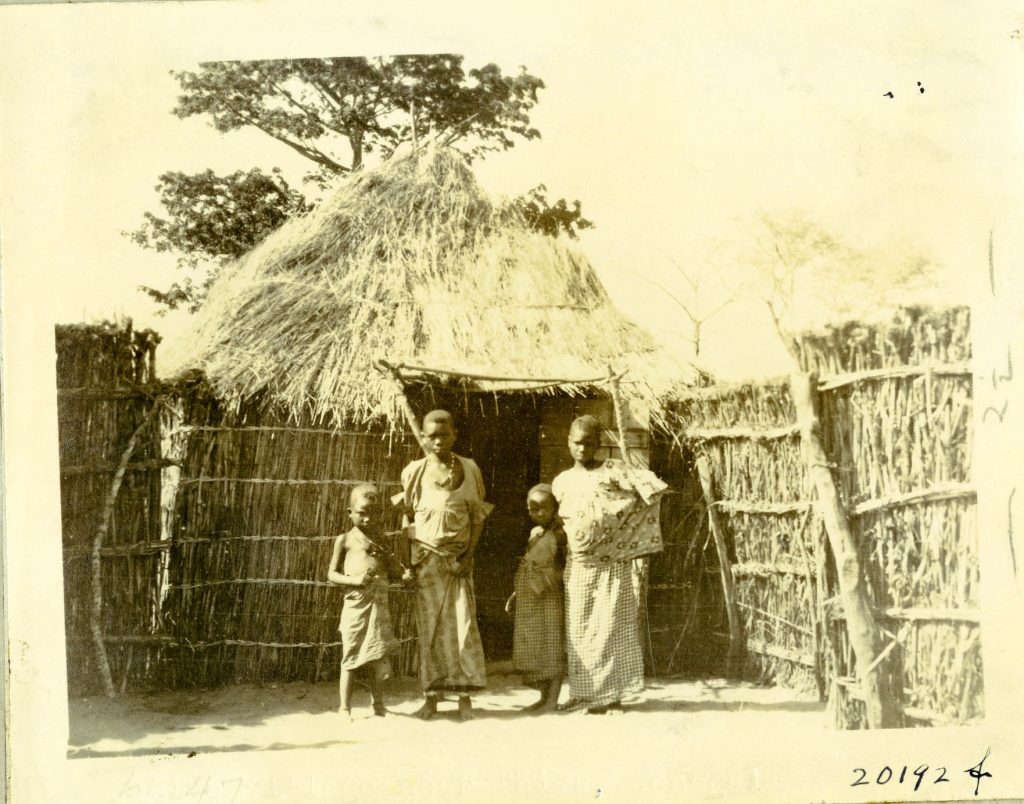
An African homestead in Thies, Sénégal. This building would have been incinerated in case of a yellow fever outbreak. Photo from the Rockefeller Archive Center.
The trials that followed, carried out under the supervision of Félix Mesnil in the French West African microbiological laboratory of Dakar, showed that although adverse effects in adults had become rarer, they remained significant. In Dakar, thirty-nine out of a hundred European test subjects developed some sort of adverse reaction, and nine subjects out of a hundred developed fevers of more than 40°C, as well as neurological symptoms.
By 1935, the first trials conducted in Paris (following Roux’s death in 1933) were also causing concern. One case, in particular, led to an international outcry.
Jacqueline B, a patient who had received the vaccine in Paris, developed narcolepsy, high fever, and neurological symptoms eleven days after the first injection. She fell into a coma for several days, stayed for three weeks at the Pasteur Hospital, and took several months to recover fully.
Following an inquiry, the Society of Exotic Pathology, the Ministry of Colonies and several high-profile scientists all recommended that the vaccine should not be deployed at scale.
A vaccine for Africa
The Pastorians had no desire to return to the drawing board. They were competing with the Rockefeller Foundation and with British researchers, who were testing their own vaccine at the Wellcome Laboratories in London.
French newspapers were eager to play up such imperial rivalries. An opinion piece entitled ‘A discovery the French did not want to make’ published in the popular satirical weekly Le Nouveau Cri, reminded people that successful vaccinations would help silence increasingly vocal critics of colonialism outraged by French massacres in Morocco and Indochina, and by the tens of thousands killed during the construction of the Congo-Ocean Railway.
‘We would stop discussing the principles of “colonialism” if these “imperialists”, the colonizers, knew how to save the colonized from the scourges, miseries, and hereditary slavery which burdens them,’
the author wrote.
‘One can colonize to empower, not to subjugate.’
Equally, by being overly cautious, the French risked becoming dependent on a British vaccine and paying an externally set price, even though in this instance ‘we are talking about vaccines, not confectionery’.2 The approval of the vaccine was not only a question of medical ethics, it was a matter of national prestige and imperial autonomy.

Time pressure and economic concerns
Laigret remained convinced that the adverse effects did not lead to permanent harm and were far outweighed by the benefits of the vaccine. In his response to the Society of Exotic Pathology, he made two arguments intended to allay concerns.
First, he claimed that the diseased tropical setting of West Africa, where the vaccine had been tested, made it all too easy to confuse common tropical illnesses with side-effects caused by the vaccination. Critics of the vaccine, he argued, were ‘giving a new interpretation to troubles which are very common in the tropics, and constitute a regular part of medical observation’.3 In Laigret’s view, there was no reason to suppose that the vaccine caused fevers and encephalitis, when any tropical disease could be behind the symptoms.
Second, Laigret suggested that instead of vaccinating French travellers to West Africa, the colonial state should undertake a mass vaccination programme in West Africa itself. His colleague, Georges Stefanopoulo, had undertaken some serological studies in West and Equatorial Africa, which suggested that Africans who had acquired childhood immunity to yellow fever could still transmit the disease to susceptible populations.
Vaccinating European travellers might protect the individuals concerned, but the danger of outbreaks requiring the introduction of quarantines, curfews and other restrictions harmful to the economy, would remain. However, a mass vaccination campaign could eradicate the disease completely.
Laigret argued that the ‘cost on economic and social life in Africa that fear of yellow fever imposes’ far outweighed the threat of harm caused by the vaccine. He insisted that ‘adverse events following yellow fever vaccination cannot be compared for an instant to the dangers of yellow fever’.4 Adverse reactions, never tolerated in Europeans, were acceptable collateral damage if triggered by a mass vaccination programme for black Africans.
Sounding the alarm
A number of Laigret’s colleagues were worried, however.
Georges Stefanopoulo, who had cultivated the original attenuated virus, expressed his concerns to colleagues at the Rockefeller Foundation, who were working on their own vaccine strain. Stefanopoulo highlighted the severity of neurological reactions in laboratory animals: nearly all the rhesus monkeys which had developed encephalitis after receiving the vaccine had ultimately died. He also feared that trial vaccinations might have caused unrecorded deaths, and wanted the international authorities to take up the matter.
As Laigret pushed for a programme of mass vaccination, Stefanopoulo became alarmed. ‘My dear Doctor Sawyer, please, I beg you, come over here to support me for a few days,’ he wrote to a Rockefeller colleague. ‘Alone, my voice is too weak’.5 Nevertheless, he was rebuffed. Rockefeller researchers were confident that their own vaccine strain would soon leave their French competitors in the dust.

Nursing school in Ayos, Cameroon, established in 1926, Institut Pasteur/Musée Pasteur.
Hell of a job
What did it mean to vaccinate an estimated sixteen million inhabitants of French West Africa, a colony seven times larger than metropolitan France?
The metropole had a developed system of clinics and hospitals, while French West Africa had very few institutions of Western biomedicine outside a few large port cities. In 1939, the federation in its entirety had about 400 qualified doctors working for the colonial public health service ‘Medical Assistance for Indigenous Peoples’,6 and fewer than ten hospitals.
It was clear that Laigret’s original design – an attenuated vaccine that required a total of three shots at intervals of several weeks – was never going to work in an African setting. Laigret needed a simpler method, even simpler than his original one-shot live virus vaccine design.
He needed a vaccine that was robust and could survive for a long time in tropical heat, as teams of vaccinators travelled to remote locations. He needed a vaccine that could be administered en masse by military troops with only the most rudimentary training.
The French had considerable experience conducting such campaigns – Eugène Jamot, another Pastorian, had become famous for his militarily run operations against sleeping sickness in Equatorial Africa. Pastorians had the necessary ambition. All they needed now was the right vaccine.
The easiest method of vaccine delivery was by scarification – superficially piercing the skin with a bifurcated needle containing a high enough dose of the vaccine to produce immunity. It was a method that had been used for administering smallpox vaccination in the French colonies for decades, familiar and easy to administer.
The downside was that it required a much higher dose of the vaccine: Laigret increased the dose of the virus in a single shot by a factor of thirty. But it got the job done. By 1939, the Pasteur Institute was reporting over 100,000 vaccinations a year in French West Africa. As the opening shots of World War II were fired in Europe, Pastorians in Dakar were preparing to launch the largest vaccination campaign in the African continent.
Invisible Africans
Surprisingly, vaccinators saw almost no adverse reactions, neurological or otherwise. The Pasteur Institute claimed that almost everyone retested ten days after receiving the vaccine had developed immunity and that none of the 1,630 control tests indicated any complications. The Pasteur Institute in Dakar reported that ‘no reaction, even slight, could be observed’ and ‘that it is currently possible to vaccinate a mass of individuals against yellow fever in minimal time’.7
Over the next few years, as World War II raged around the globe, this is exactly what the Pasteur Institute did. By the time the war ended, the institute was claiming to have vaccinated over 14 million people – nearly the entire population of the colony.
If you dig deeper into the archives, however, the picture becomes murkier. Reports by doctors overseeing work at the Pasteur Institute, held in the laboratory’s Dakar archives, paint a picture of frustrated supervisors and difficult campaigns.
Vaccination sites were often located far from people’s homes and required Africans to travel dozens of miles from their native villages to receive shots. Because the vaccine was administered via scarification, many subjects did not realize they were being vaccinated against yellow fever, rather than smallpox. Few wanted to return for control tests.
One doctor, who supervised vaccinations in the Ivory Coast village of Brinndoukrou, reported that Africans, ‘having been vaccinated some days earlier, did not understand why they were being forced to travel again’.8 Dr Peltier, the lead vaccinator, was equally frustrated, writing that Africans ‘had a hard time understanding the reasons for control tests, and made little effort to participate in such efforts’.9 One can imagine that people who did develop a fever were even less likely to travel miles for a check-up they did not understand.
A second problem made it even less likely to observe adverse reactions. The Pasteur Institute was pressed for time. Even with help from the military, teams of vaccinators had to move quickly to reach the diverse regions of French West Africa.
Consequently, control tests were scheduled for ten days after the initial vaccination. But as earlier trials done in Tunis and Dakar had shown, adverse effects usually presented themselves around fourteen days after the initial injection.
So even if African subjects did develop fevers or meningitis, their symptoms would have manifested too late for them to be registered by Pastorian observers. By then the vaccinators would have left for their next destination.
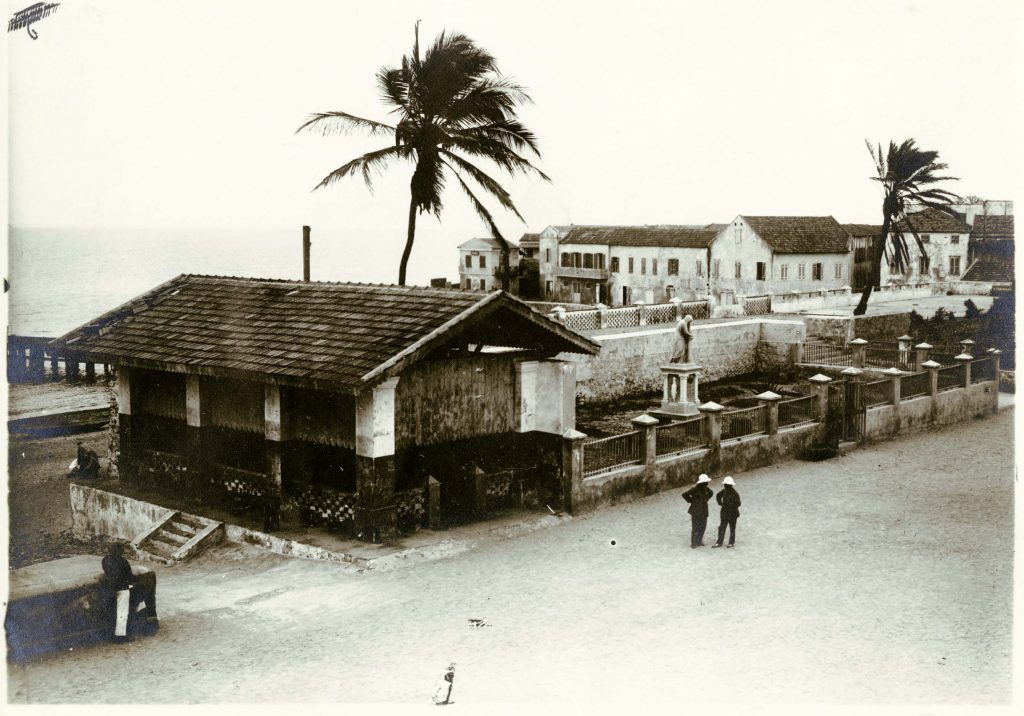
French constructions in Dakar. Two men standing in front of a memorial to those perished in the 1878 yellow fever epidemic, circa 1928. Rockefeller Archive Center.
A difference in treatment
There are indications that the vaccine used in the West African campaigns did cause harmful outcomes. In 1941, the Pasteur Institute reported adverse side-effects in European recipients, vaccinated at the Dantec hospital in Dakar.
But, for Europeans, the institute had developed a long list of contraindications to the vaccination. These included acute illness, ongoing fevers, chronic ailments, liver or kidney problems, and ‘in general terms, any condition that diminishes the resistance of the subject’. European children were also exempt. Even given these constraints, reports of adverse effects in Europeans continued to surface.
For Africans, the only ‘temporary contraindication’ was ‘acute fever’.10
After the war, UNRRA tested the vaccine on six hundred French soldiers, who were told to stay away from military activity and rest for a week after receiving the vaccine. Nonetheless, some 12 per cent of them had some sort of ‘febrile or encephalitic reaction’.
Due to an ‘error’, however, one group went on a fifteen-kilometre march in the open sun after being vaccinated – not unlike the African subjects who had been obliged to travel for vaccination during the war. More than 35 per cent of soldiers in this group experienced some sort of reaction to the vaccine.
As early as 1934, Georges Stefanopoulo had written to colleagues at the Rockefeller Foundation pleading them to intervene:
‘The vaccine is unfortunately supported by characters who are not afraid to kill some of their fellow creatures to gain experience, and particularly to infect people from Black African populations who remain outside “statistical data”’.11
The consequent pressure pushed Laigret to modify his vaccine. But Africans did remain outside statistical data. The shortage of hospitals, medical personnel and roads, which made following proper testing protocols all but impossible, meant that adverse effects went unreported during the first year of the vaccination campaign in 1939.
Accordingly, the vaccine was approved and rolled out. It was not until decolonization, in the late 1950s and 1960s, that disastrous vaccination programmes once again highlighted the risks associated with the French vaccine strain.
The long twilight of a vaccine
Several decades and forty million vaccinations later, the side-effects and deaths associated with the French strain forced the WHO to recommend that the vaccine should not be administered to children, except in public health emergencies. Finally, in the 1980s, as the Rockefeller Foundation’s 17-D vaccine improved, the Dakar vaccine was discontinued.
The number of lives lost in the wartime vaccination campaigns will never be known, although the immunologist Hervé Bazin has estimated that as many as three thousand people may have died. By way of comparison, the infamous failure of the Cutter Laboratories to manufacture the Salk polio vaccine correctly in 1955 led to ten deaths. Yet the incident reshaped the American pharmaceutical industry for decades.
The trajectory of the Dakar yellow fever vaccine reveals the role microbiological engineering and colonial infrastructure played in obscuring the vaccine’s harmful effects. When critics in France raised concerns about the vaccine’s safety, Jean Laigret repurposed the vaccine for a mass roll-out in Africa.
Delivery efficiency was prioritized over safety. During the vaccination campaigns, a lack of medical infrastructure, the rush to immunize everybody in French West Africa and lax record-keeping rendered any data on adverse reactions, gathered from control tests, well-nigh invisible.
Only a few Europeans in well-resourced hospitals reported fevers and neurological symptoms. But it was wartime. They recovered and the cases were forgotten.
Jean Laigret was shocked when he witnessed the tragedy in Enugu, Nigeria in 1952. He should not have been. As Stefanopoulo had predicted decades earlier, poor colonial infrastructure and the insistence of the Pasteur Institute on rapid vaccination roll-outs ensured that African patients who suffered as a result were left wholly excluded from statistical data.
This essay is adapted from Aro Velmet’s book, Pasteur’s Empire: Bacteriology and Politics in France, its Colonies, and the World, published by Oxford University Press, 2020
Jean Laigret, “Hommage à Jean Laigret, la petite histoire de la découverte de la vaccination contre la fièvre jaune,” [A tribute to Jean Laigret: the story of how the yellow fever vaccine came to be discovered], La Presse Médicale, 5 November 1966, 2441
Maurice Prax, “Une découverte que les français ne voulaient pas… découvrir” [A discovery the French did not want to make], Le Nouveau Cri, 8 September 1934
J. Laigret, “Au sujet des réactions nerveuses de la vaccination contre la fièvre jaune” [On reactions to the yellow fever vaccine affecting the nervous system], Bulletin de la Société de Pathologie Exotique, 14 October 1936
J. Laigret, “De l’interprétation des troubles consécutifs aux vaccination par les virus vivants, en particulier à la vaccination de la fièvre jaune” [Interpreting side-effects arising from live virus vaccines, particularly the yellow fever vaccine] Bulletin de la Société de pathologie exotique et de ses filiales, 11 March 1936, 230
Georges Stefanopoulo to Dr. Sawyer, 16 October 1934, Folder 313, Box 28, Series 4 IHB/D, RG 5, Rockefeller Archive Center, Sleepy Hollow, NY
French: Assistance Médicale Indigène
Médecin Lt. Col Durieux, “Rapport sur la mission de vaccinations effectué en Côte d’Ivoire” [Report on the vaccination mission carried out in the Ivory Coast], undated; M. Peltier, “Vaccination antiamarile, simple ou associée à la vaccination antivariolique” [The yellow fever vaccine: single or combined with the smallpox vaccine], undated, IP.DIR.5, Archives of the Pasteur Institute, Paris
Médecin-Capitaine Bergouniou to Chef du Service de Santé à Abidjan, Official Report, 17 April 1940, IP.SER.3, Archives of the Pasteur Institute of Dakar, Dakar
‘Vaccination mixte contre la fièvre jaune et la variole sur des populations indigènes du Sénégal’ [Effects of combined vaccines against yellow fever and smallpox on the indigenous populations of Senegal], 15, IP.DIR.5, Archives of the Pasteur Institute of Dakar, Dakar
“Instruction pour l’application de l’arrêté du 10 septembre 1941 rendant obligatoire la vaccination anti-amaryle en Afrique Occidentale Française” [Instruction for the implementation of the decree dated 10 September 1941 rendering anti-amaryl vaccination compulsory in French West Africa], Archives of the Pasteur Institute of Dakar, Dakar
Georges Stefanopoulo to Dr. Sawyer, 16 October 1934, Folder 313, Box 28, Series 4 IHB/D, RG 5, Rockefeller Archive Center, Sleepy Hollow, NY
Published 31 March 2021
Original in English
First published by Eurozine
© Aro Velmet / Eurozine
PDF/PRINT

Invest in insight!
After over 20 years of publishing for free, Eurozine needs your support to get through an exceptionally lean year.
Become a Patron and get exciting perks for your help!
![]()

Want to hear a human voice?
Listen and subscribe wherever
you get your podcasts.
Newsletter
Subscribe to know what’s worth thinking about.
Related Articles



Related Articles

In France, the censorship of pro-Palestinian positions is particularly severe, with antisemitism accusations increasingly being used by the far right. But behind the current wave of repression lies a set of attitudes that are neither new, nor exclusively rightwing.

Touted as Europe’s largest infrastructure project, the Grand Paris Express promises better connectivity and improved public transport for the French capital. However, for Roma squatters and slum residents, the colossal project has meant forced evictions and further exclusion from society.